Heroin Information, History and Statistics

Heroin is a powerful narcotic that is processed from morphine. Morphine is a naturally occurring substance that is extracted from the seed pod of various opium poppy plants. Poppy seeds used in baking are grown from the same plant as the opium is harvested from. Depending on where the poppy seeds are harvested, it’s possible for the seeds to become contaminated with the opium extract. This can result in failed drug screens, as one suburban mother found out. However, it’s unlikely that the amount of opium extract in the poppy seeds are enough to produce a euphoric, and therefore addictive, effect.
While it might seem that the relative ease with which poppy seeds can be acquired would make it a commonly grown plant, much as we see with illicit marijuana, in fact, an article from Scientific American from 1869 shows that opium poppy was once cultivated in the United States. However, the classification by the DEA of the raw plant as a Schedule II substance and its robust domestic enforcement has curtailed home opium farms to a point where a recent bust in North Carolina was one of only two in the nation. In addition to legal issues, the plant requires a lot of space to produce enough raw opium to turn a profit when imported heroin is much cheaper.
In the United States, when opium is made into heroin it is classified as a Schedule I drug by the Drug Enforcement Agency (DEA): “Schedule I drugs, substances, or chemicals are defined as drugs with no currently accepted medical use and a high potential for abuse.“ Heroin is most commonly used for its euphoric effects. It is usually injected and can also be inhaled, smoked or snorted. The onset of the effects is rapid and last for a few hours. Heroin is highly addictive and users rapidly develop a tolerance of the drug, needing more and more to obtain the same effect. Heroin produces compulsive, drug-seeking and drug-taking behavior. Heroin use is known to cause major medical complications, which can include respiratory depression or failure, constipation, insomnia, collapsed veins, abscesses, bacterial infections, and blood-borne diseases such as hepatitis and HIV. Injection drug use is currently the most common means of transmitting hepatitis in the United States.
Physical Properties of Heroin


(Images courtesy of the DEA.)

Heroin ranges in color from white to dark sticky, tar-like substances. While the pure form of the drug is white, impurities during the production of heroin cause it to appear similar to black pitch or tar. Within this range, there is a wide variety of different colors and textures, all relating to how the heroin was produced. While heroin in its purest form has no smell and a bitter taste, when burned, heroin has a distinct pungent odor with a dark chemical taste when inhaled.
Common questions about the physical properties of Heroin:
What does heroin look like? Heroin ranges in color from pure white to a sticky black or brown substance and can appear as a fine powder or course, sticky sand- or tar-like substance.
What does heroin taste like? Heroin in its pure form is bitter, but it can have a chemical taste when burned.
How is heroin sold?—Heroin is most commonly sold in little plastic baggies, small glassine pouches or balloons.
Where does heroin come from?—There are three primary geographic sources of illicitly grown poppies which are used to produce heroin:
- The Golden Triangle, including Myanmar, Thailand and Laos.
- Southwest Asia, including Afghanistan, Pakistan and Iran.
- Mexico, Colombia and Guatemala.
The geographic source of origin determines how the heroin is harvested, processed, and in which form, and where it is eventually distributed.
The Heroin Trade in the United States
In 1937 at Marseilles, France, there was a discovery of heroin labs controlled by the infamous Corsican gang leader Paul Carbone. These labs were constructed as part of a vast French smuggling network that trafficked heroin and which mainly targetted the U.S. This network came to be known as “the French Connection.”
Prior to the 1970s, Turkey supplied the majority of the raw materials that were then turned into heroin in the Corsican labs. Turkey had long been responsible for providing opium to medical suppliers, however many of the farmers had no problem selling excess crops to the underground heroin trade. This provided the perfect source for the gangs in Marseilles, and with easy access to seaports and shipping, the French Connection began to increase production, targeting the United States.
The escalation of heroin smuggling is documented in DEA history books. On February 5th, 1947, 4 pounds of heroin were seized from a passenger coming from Marseilles. On March 27th, 28 pounds were seized and on January 7th, 50 pounds were seized. By 1960 it is estimated that between 2,600 and 5,000 pounds of heroin were coming into the United States from France annually, and by 1969 the French Connection was supplying up to 90% of the heroin in the United States.
In 1971, President Nixon launched the “War on Drugs” campaign, and with it came increased pressure on Turkey to ban poppy production. Later that year, Turkey acquiesced and agreed to ban the cultivation of heroin, which went into full effect in 1972. At the same time, a major operation was running and succeeded in breaking up the French Connection—a major distribution channel of heroin from Turkey to the US. However, in 1974 Turkey restarted state-licensed production of opium under the UN International Narcotics Control Board.
While the primary supply for heroin was cut off, the demand for heroin in the United States was not addressed. The shortage of heroin that was created by the “War on Drugs” operation was compensated with methadone and new supply routes that were established from Southeast Asia and Mexico. This shift allowed drug production to move closer to home, with Mexico now providing the majority of heroin to the United States.
The Scope of Heroin Use in the United States
According to the 1996 National Household Survey on Drug Abuse, an estimated 2.4 million people used heroin at some time in their lives, and nearly 216,000 of them reported using it within the month preceding that survey. This represented 141,000 new heroin users since the previous year and had been an increasing trend since the beginning of the decade. A large proportion of these new users were smoking, snorting, or sniffing heroin, and most were under age 26. Estimates of use for other age groups also increased, particularly among youths age 12 to 17. The incidence of first-time heroin use among this age group increased fourfold from 1980 to 1995.
The 1996 Drug Abuse Warning Network (DAWN), which collects data on drug-related hospital emergency department (ED) episodes from 21 metropolitan areas, estimates that 14 percent of all drug-related ED episodes involved heroin. Even more alarming is the fact that between 1988 and 1994, heroin-related ED episodes increased by 64 percent (from 39,063 to 64,013).
But these early signs of a pending disaster were largely ignored despite NIDA’s Community Epidemiology Work Group (CEWG), which provides information about the nature and patterns of drug use in 20 cities. It reported in its December 1996 publication that statistics from drug-abuse treatment admissions in Newark, San Francisco, Los Angeles, and Boston found heroin to be the primary drug of abuse, and it ranked a close second to cocaine in New York and Seattle.
In December 1996, CEWG reported that the availability of low-priced, high-quality heroin continued to increase, especially in the East and some areas of the Midwest. This increase was also reported in some cities that previously had escaped the influx of high-quality heroin.
Quantitative indicators and field reports continue to suggest an increasing incidence of new users (snorters) in the younger age groups, often among women. One concern is that young heroin snorters may shift to needle injecting because of increased tolerance, nasal soreness, or declining or unreliable purity. Injection use would place them at increased risk of contracting HIV/AIDS.
In some areas, such as Boston and San Francisco, the recent initiates increasingly include members of the middle class. In Newark, heroin users are usually found in suburban populations.
The Growing Storm of Prescription Drug Abuse
As the supply of heroin began to increase and trade routes were established between Mexico and the United States a growing storm was on the horizon. In the late 1990s, prescription-drug companies began to market powerful painkilling drugs to the medical community, assuring them that the drugs had little chance of being addictive. This led to healthcare providers prescribing the drugs at an ever-increasing rate. These prescriptions were a double-edged sword. Not only did the patients become addicted to these powerful pain killers, the drugs were often diverted to street users who also became addicted to the drugs. By the 2000s it became clear that thousands of people were dying from prescription-drug misuse, and the reaction to crack down on the prescriptions may have stemmed the tide temporarily. However, a lack of resources to provide effective treatment created the perfect storm for addiction to grow. Individuals who had become addicted under a doctor’s care were now cut off and the availability of these drugs on the street plummeted.
With the establishment of heroin trade routes in the 1970s after the folding of the French Connection, gangs in Mexico were perfectly poised to fill the demand for heroin created by the vacuum left by the crackdown on opioid prescriptions. The result was that by 2017 an estimated 1.7 million people suffered from substance- use disorders relating to opioids, with 652,000 people hooked on heroin. The so-called “War on Drugs” had fueled an epidemic with few solutions in sight.
Current Heroin-Use Statistics
Internationally heroin is the most used opiate:
- 12 to 13 million users consume an estimated 375 tons of heroin each year (equal to 2,800 tons of opium), making heroin the most abused opiate worldwide.
- As of 2011, the UNDOC estimated that there are between 10,000 and 12,000 tons of opium held in stockpiles—which is enough to fulfill the worldwide demand of opium and heroin for at least three years.
- An estimated 948,000 individuals reported using heroin within the past year.
The demand for heroin is not lessening and all the while the deaths from heroin continue to increase.
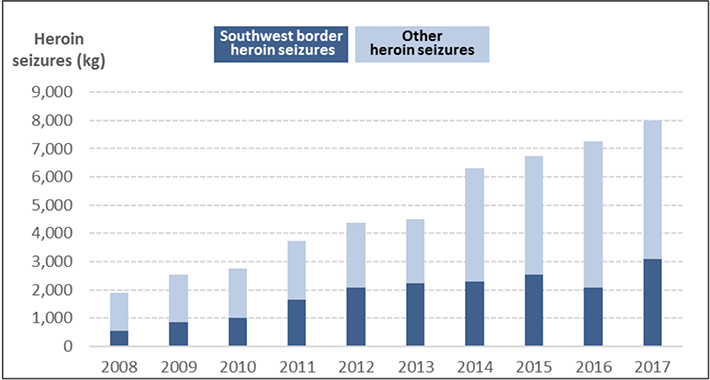
- Seizures of heroin across the United States have been increasing over the past decade. 7,979 kilograms (17,590 pounds) of heroin were seized in 2017.
- According to recent drug overdose death statistics in the United states, there were 15,469 heroin-related deaths—an increase of 19 percent from 2015. Deaths from heroin have continued to increase every year since 2010.
For More Information on Heroin:
- Signs and Symptoms of Heroin Use
- Heroin Drug Abuse
- Heroin Addiction, Recovery, Rehabilitation and Treatment
Sources used:
- https://www.history.com/topics/crime/history-of-heroin-morphine-and-opiates
- https://www.dea.gov/sites/default/files/2018-07/1970-1975%20p%2030-39.pdf
- https://www.drugabuse.gov/drugs-abuse/opioids/opioid-overdose-crisis
- https://beta.washingtonpost.com/news/morning-mix/wp/2018/08/08/yes-you-can-fail-a-drug-test-by-eating-a-poppy-seed-bagel-as-a-maryland-mother-learned/
- https://www.ncbi.nlm.nih.gov/pubmed/12555905
- https://www.dea.gov/sites/default/files/2018-11/DIR-032-18%202018%20NDTA%20final%20low%20resolution.pdf
- https://fas.org/sgp/crs/misc/R44599.pdf
Reviewed and Editeb by Claire Pinelli, ICAADC, CCS, LADC, MCAP, RAS